GLP-1 and GIP: a new opportunity in sleep apnea (OSA)
What is OSAS?
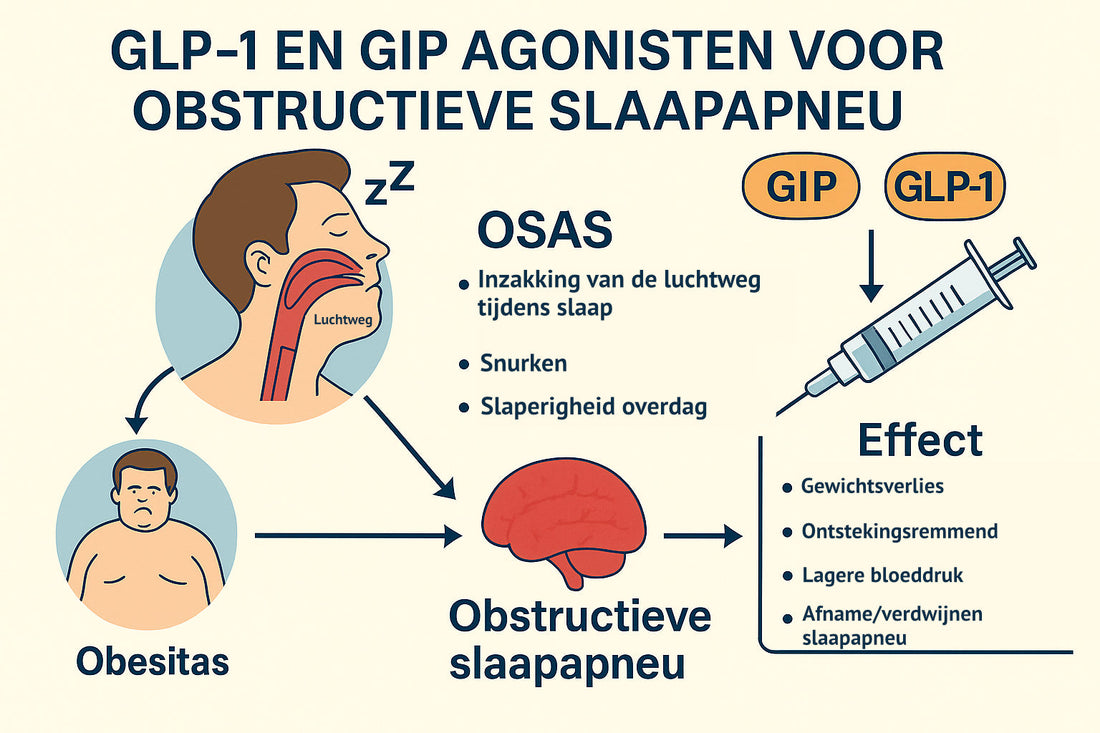
Obstructive Sleep Apnea Syndrome (OSAS) is a condition in which the throat repeatedly closes during sleep. This causes breathing to stop dozens of times an hour. This not only leads to loud snoring and daytime fatigue, but also increases the risk of cardiovascular disease, high blood pressure and diabetes (1).
More than 900 million people worldwide have OSAS, of which about 40% have a moderate to severe form (1). In the Netherlands, this number amounts to several hundred thousand people. The standard treatment is often a CPAP device, which uses air pressure to keep the airway open. While this can be effective, many people find it difficult to use it consistently every night.
Why does obesity play such a major role in OSAS?
Excess weight – and especially fat around the abdomen and neck – is one of the main causes of OSAS.
-
Fat around the airway can narrow the throat, causing it to close more quickly.
-
Belly fat puts increased pressure on the lungs and chest, making breathing more difficult during sleep.
-
In addition, obesity causes a low-grade inflammatory response in the body, which puts extra strain on the respiratory and cardiovascular systems (1).
Losing weight reduces the risk of apnea. Guidelines often recommend a weight loss of 7–10%. However, in practice, this is difficult to maintain with lifestyle changes alone. This is where new medications come into play.
What are GLP-1 and GIP?
GLP-1 (glucagon-like peptide-1) and GIP (glucose-dependent insulinotropic polypeptide) are hormones that our bodies produce after a meal. They have several effects:
-
They stimulate the release of insulin when you eat.
-
They slow down stomach emptying → you feel full faster.
-
They work in the brain and provide a stronger feeling of satiety.
New medications mimic these hormones. Well-known examples include:
-
Semaglutide (Ozempic) – a GLP-1 agonist.
-
Tirzepatide (Mounjaro) – works on both the GLP-1 and GIP receptors.
These agents produce an average weight loss of 15–20% in a year – comparable to some bariatric surgeries (1).
How do GLP-1 and GIP affect sleep apnea?
The link between these agents and OSAS is on several levels:
-
Weight loss: less fat around the throat and abdomen reduces the chance of breathing stops.
-
Anti-inflammation: GLP-1/GIP reduce inflammatory substances such as CRP, which may benefit the airways and blood vessels (1).
-
Lowering blood pressure: high blood pressure and OSAS reinforce each other, and this effect can be partly reversed.
-
Possible direct effect: Some studies suggest that GLP-1 also directly influences breathing regulation in the brain (2).
What does science say?
Previous insights
Even before the advent of tirzepatide, it was suspected that GLP-1 agonists could improve OSAS. Small studies with liraglutide and semaglutide already showed a decrease in the Apnea-Hypopnea Index (AHI) , primarily due to weight loss (2,3).
The SURMOUNT-OSA study (2024)
The major breakthrough came in 2024 with the SURMOUNT-OSA study , published in The New England Journal of Medicine (1).
-
Design: 469 people with obesity (average BMI 39) and moderate to severe OSAS participated. Half used CPAP, the other half did not.
-
Treatment: weekly injections of tirzepatide (10–15 mg) or placebo, for 52 weeks.
-
Outcome measure: change in AHI (number of breathing pauses per hour).
Results:
-
With tirzepatide the AHI decreased by 25–29 respiratory arrests per hour , with placebo only 5.
-
After one year, almost half of the patients had an AHI <15, meaning no or only mild sleep apnea.
-
Body weight decreased by an average of 18–20% .
-
Blood pressure, inflammation values (CRP) and oxygen deficiency load during sleep also decreased.
-
Patients reported less drowsiness and better sleep.
Side effects:
-
Mainly gastrointestinal complaints (nausea, diarrhea, constipation).
-
Generally mild to moderate and especially in the first few weeks.
What does this mean for the treatment of OSAS?
Until now the options for OSAS were:
-
CPAP (effective, but difficult to maintain).
-
Braces or jaw surgery (in some patients).
-
Weight loss (difficult to achieve long-term).
With GLP-1 and GIP drugs, for the first time, a drug treatment has been developed that not only suppresses the symptoms, but directly addresses the cause, namely obesity .
This can have major consequences:
-
For patients who cannot tolerate CPAP.
-
For people with severe obesity who are at high risk for OSAS.
-
As a supplement to existing treatments.
What are the possible disadvantages and points of concern?
Although the results are promising, there are also limitations and concerns:
-
Not suitable for everyone: The studies were conducted in people with obesity and moderate to severe OSAS. It is not yet known whether these medications also work in people of normal weight (1).
-
Costs and reimbursement: Tirzepatide is expensive and is currently often only reimbursed for diabetes. Reimbursement for sleep apnea without diabetes is still uncertain (4).
-
Long-term effects still unclear: It has not yet been proven whether these agents also reduce the risk of cardiovascular disease or death in the long term. Additional research is currently underway into this (1).
-
Side effects: The most common are gastrointestinal complaints such as nausea, diarrhea, or constipation. Rare, but more serious, side effects include pancreatitis (1,2).
Conclusion
GLP-1 and GIP agonists, such as tirzepatide, are a promising new treatment option for sleep apnea. They address the root cause of the problem – excess weight – and thus improve both the severity of OSAS and associated risk factors such as high blood pressure and inflammation.
For patients this may mean:
-
Fewer breathing pauses per night.
-
Better sleep and more energy during the day.
-
Lower risk of cardiovascular problems.
Although the drugs are not yet available to everyone, this appears to be a real breakthrough in the treatment of OSAS . The coming years will reveal how these medications can be used alongside or instead of CPAP and surgery.
References
-
Malhotra A, Grunstein RR, Fietze I, et al. Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity . N Engl J Med. 2024;391:1193-205.
-
McSharry DG, Malhotra A. Potential influences of GLP-1 receptor agonists on sleep apnea pathophysiology . Curr Opin Pulm Med. 2021;27(6):495–500.
-
Grunstein RR, Stenlöf K, Hedner J. Obesity and obstructive sleep apnea: pathogenic mechanisms and therapeutic approaches . Sleep Med Rev. 2014;18(5):341-349.
-
Diabetesgeneeskunde.nl. Tirzepatide improves symptoms of sleep apnea (2024).